
You’ve seen the ad. Tired, foggy, less interested in everything, and one neat fix waiting on the other side of a ten-question quiz and your credit card number. Before you tap “start,” let’s talk about what you’re actually buying, because “TRT clinic” is a label three very different businesses hide behind, and the cheapest one on your feed is almost never the one doing the actual work.
Here’s the deal up front, because it changes how you should read everything else in this article. Testosterone therapy is a prescription treatment for a diagnosed medical condition. It is not a supplement, it is not a life hack, and it is not something a quiz can responsibly hand out. Nothing in this piece tells you what to take. It tells you the tricks to watch for, and the questions to put to the licensed clinician who should be the one making that call with your actual labs on the screen.
The trap: one product marketed as the whole solution
Most of these ads are selling you one tool and pretending it’s the only tool. It isn’t. There are three, and which one fits you depends entirely on your situation, something a quiz cannot know and a single-product shop has no incentive to ask about.
The first is testosterone replacement itself, the actual treatment for hypogonadism (a body that isn’t making enough on its own). It’s usually an injection, testosterone cypionate or enanthate, sometimes a cream or gel. It works by replacing the hormone directly, and here’s the part the glossy landing page conveniently leaves off the label: it also tells your body to stop making its own. We’ll come back to why that matters.
The second is enclomiphene, the option nobody advertises because it doesn’t fit the “shot in your fridge” fantasy. Instead of adding testosterone from outside, it nudges your own brain to tell your testicles to make more. In a randomized phase II trial against a topical testosterone gel in men with secondary hypogonadism, enclomiphene raised serum testosterone about as well as the gel while also raising LH and FSH and, crucially, conserving sperm counts, the exact thing standard replacement tends to tank [4]. One thing worth flagging before you shop: enclomiphene isn’t FDA-approved. It’s prescribed and prepared through compounding pharmacies under a valid prescription, and a straight-shooting provider will tell you that outright instead of burying it [5].
The third is HCG, which acts like LH and keeps the testicles running while you’re on testosterone therapy. A 2025 real-world analysis looked at men who’d suppressed their own production using non-prescribed androgens, and found HCG substantially restored sperm output, with the share hitting a normal total motile sperm count jumping from 5 percent to 58 percent after treatment (though some men still landed below normal) [6]. That single number is exactly why a legitimate clinic stocks more than one option, and why your family plans need to be in the very first conversation, not an afterthought.
So the real question isn’t “what’s the best TRT clinic.” It’s “who can actually route me to the right tool for my situation.” A man who’s done having kids and a man who wants to protect his fertility need two different protocols. Anyone selling you only one product cannot give you both, no matter how good their branding is.
Who this is for, and who’s being sold a fantasy
Here’s the blur the ads work hard to keep blurry. Testosterone therapy is for men with a diagnosed, confirmed deficiency, not for any man who’s tired and Googling at 11pm.
The Endocrine Society’s clinical practice guideline doesn’t leave wiggle room: testosterone should be prescribed only to men who have both symptoms and unequivocally low testosterone, confirmed by repeating a fasting morning blood draw rather than acting off one borderline lab [1]. The FDA backs this from the regulatory side too. Approved testosterone products are indicated for hypogonadism tied to an actual medical condition, and their benefit and safety have not been established for low testosterone that’s simply due to aging [5].
Read that twice. It’s the cleanest filter you own. If your levels are normal, the evidence doesn’t support taking testosterone to chase more energy, and a provider willing to write that script anyway is telling you exactly how it runs its business. The men who genuinely benefit are the ones with a real, confirmed deficiency. If that’s not you, the honest answer might be that a hormone isn’t the fix for what’s going on.
What it actually does (spoiler: less than the pitch)
Say your deficiency is real and confirmed. What can you actually expect? The honest answer is narrower than the ad copy.
The best evidence comes from the Testosterone Trials, a coordinated set of placebo-controlled trials in 790 men aged 65 and older with low testosterone, published in the New England Journal of Medicine in 2016 [2]. The clear wins were in sexual health: treatment significantly improved sexual activity, desire, and erectile function versus placebo, with a modest bump in mood. Physical function was murkier, improving when the trials were pooled but not reaching significance in the dedicated physical-function trial on its own.
Now the part that should reset your expectations entirely. In those same trials, testosterone showed no significant benefit for vitality, measured on a standard fatigue scale [2]. That’s the honest rebuttal to nearly every “feel young again” ad you’ve scrolled past. In the best study we’ve got, in men who genuinely had low levels, it did not move the fatigue needle. So here’s the accurate version: testosterone reliably helps sexual function and modestly helps mood in men who are truly deficient. The energy promise is the part the data didn’t deliver.
The safety picture, and the fine print they skip
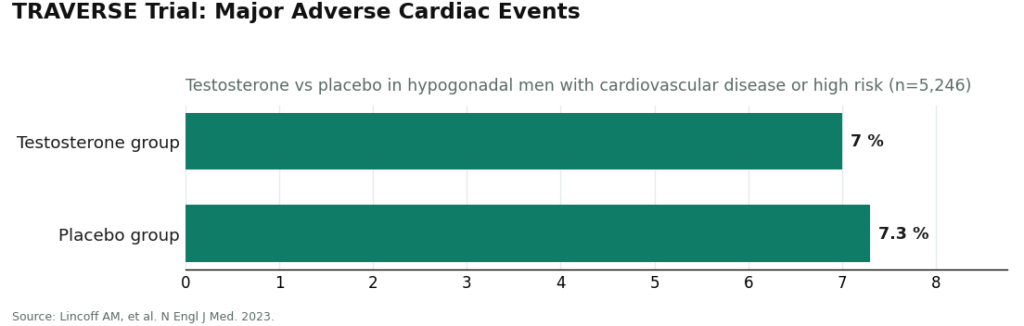
For years the big open question was the heart, and a large trial has now mostly answered it, for men who are actually being monitored. TRAVERSE, published in the New England Journal of Medicine in 2023, enrolled 5,246 men aged 45 to 80 with hypogonadism who already had, or were at high risk for, cardiovascular disease [3]. The headline finding was reassuring: testosterone was noninferior to placebo for major adverse cardiac events, with a primary event rate of 7.0 percent in the testosterone group versus 7.3 percent on placebo. Following TRAVERSE and related post-market data, the FDA updated testosterone labeling, removing the boxed cardiovascular warning while adding a new warning about increased blood pressure [5].
But that same trial is exactly why supervision still earns its keep, and this is the part the sales page never quotes. TRAVERSE also found higher rates of atrial fibrillation, acute kidney injury, and pulmonary embolism in the testosterone group [3]. That’s not a reason for a man who genuinely needs treatment to avoid it. It’s the specific list a supervising clinician is watching for, which is the whole reason follow-up labs exist as a safety net rather than paperwork for its own sake. Stack the fertility effect on top, since outside testosterone suppresses your own production and can lower sperm count, and you get a clear job description for a legitimate provider: confirm the diagnosis, set the dose, and keep watching the things that need watching.
Here’s how they get you
Now let’s name the tricks, one at a time, because once you see them you can’t unsee them.
The trick: a quiz stands in for bloodwork. You answer some questions about energy and mood, and a prescription appears with no draw ever taken. The tell: the guideline is explicit that diagnosis requires unequivocally low testosterone confirmed by a repeated fasting morning measurement [1]. If nobody’s drawn your blood, nobody has actually diagnosed you with anything.
The trick: the flat monthly fee. It sounds simple and reassuring, and it tells you almost nothing. The tell: a cheap subscription and a thorough clinic can charge nearly identical money. The difference is entirely in whether the safety work is happening behind that number, not in the number itself.
The trick: a vial labeled “research use only,” no labs required, no dose discussed, and a disclaimer that walks the seller away clean if the contents don’t match the label. The tell: the hormone might read the same on paper as a prescribed version, but one route comes wrapped in the monitoring a real guideline calls for, and the other comes wrapped in fine print warning you it was never meant for a human body. There’s nothing to weigh there. Walk.
The trick: the clinic that only sells one product, so it prescribes it to everyone regardless of whether you’re trying to have kids in five years. The tell: ask directly what happens to your fertility. A shop that can only offer testosterone, with nothing for men who want to preserve sperm count, has already told you it’s not built around your actual situation.
The trick: never getting your blood re-drawn after the first script. The tell: the guideline calls for structured first-year monitoring, including repeat testosterone, hematocrit, and a prostate-risk evaluation [1]. A provider that writes one script and disappears cannot possibly be doing that. This, more than the price tag, is the single clearest sign you’re dealing with a vending machine instead of a clinic.
The legitimate route
If you’d rather not sort all of this out solo, it helps to have one concrete example of what the supervised lane actually looks like in practice. FormBlends operates inside that lane: physician-supervised telehealth where a licensed clinician reviews your profile first, any prescription follows that review, and whatever gets prescribed is filled through a licensed 503A compounding pharmacy. I’m naming it as a worked example of the model, nothing is for sale here, and this isn’t a ranked buying guide. It earns a mention because it shows what the setup looks like when oversight, sourcing, and follow-up get built in from day one instead of stripped out to hit a lower price.
What that oversight layer adds on top of compounding, specifically, is a clinician actually reading your history, real labs driving the decision, a licensed pharmacy doing the dispensing, and follow-up testing steering any changes. None of that exists the moment you self-source from a vial with no name attached to it.
The bottom line
You’re not shopping for the lowest monthly fee. You’re shopping for a provider that confirms a real diagnosis with actual labs, keeps a clinician involved in your dose, follows up with you over time, and tells you straight that testosterone helps sexual function and mood in genuinely deficient men rather than promising it’ll make you feel twenty again. If your levels are normal, the honest answer might be that you don’t need any of this. If they’re genuinely low, the honest answer is supervision, not whichever vial ships fastest.
Answers to the common questions
Is one low blood test enough to start TRT? No, and if a provider says otherwise, that’s your red flag. The Endocrine Society guideline requires confirming an unequivocally low value with a repeated fasting morning measurement before any prescription, because testosterone swings through the day and a single borderline reading tells you very little [1]. A provider prescribing off one number, or off a quiz with no draw at all, has skipped the first step the guideline demands. That tells you most of what you need to know about how they operate.
Does TRT actually fix low energy and fatigue? Not reliably, and this is the gap between the ad and the data. In the Testosterone Trials, the best placebo-controlled evidence we have, testosterone showed no significant benefit for vitality on a standard fatigue scale, even in men who genuinely had low levels [2]. The consistent wins were sexual desire, sexual activity, and erectile function, plus a modest mood lift. The “feel young again” energy pitch is the part the evidence just doesn’t back up.
If I want kids someday, is standard testosterone the wrong move? Often, yes, and this is where a single-product shop will steer you wrong. Injected or topical testosterone tells your body to stop making its own and tends to suppress sperm production, which is why fertility-minded men often get routed to enclomiphene instead, which raised testosterone about as well as a gel while conserving sperm counts in a phase II trial, or to HCG as an add-on [4][6]. The right call depends on your family plans, which is exactly why that conversation needs to happen up front, and exactly why a provider stocking only one option can’t tailor anything to you.
Is the heart risk with TRT settled now? Largely, for men who are actually monitored. TRAVERSE enrolled over 5,000 hypogonadal men with cardiovascular disease or high risk and found testosterone noninferior to placebo for major cardiac events, which is why the FDA pulled the boxed cardiovascular warning [3][5]. That same trial flagged higher rates of atrial fibrillation, acute kidney injury, and pulmonary embolism, which is exactly why a supervising clinician and repeat labs still earn their place in this.
Why is the “research use only” testosterone so much cheaper? Because the price reflects what’s missing, not a discount. A research-chemical seller screens you for nothing, sets no dose, runs no follow-up labs, and disclaims responsibility for what’s actually in the vial. The hormone might be nominally the same compound, but the lower price comes from stripping out the diagnosis, the supervision, and the accountability that make the treatment safe in the first place.
What’s the one giveaway of a bad TRT provider? It never re-draws your blood. Structured first-year monitoring, including repeat testosterone, hematocrit, and a prostate-risk evaluation, is baked into any guideline-aligned clinic, and one that prescribes once and vanishes simply cannot deliver it [1]. The price tag tells you almost nothing here. Whether they keep testing you over time tells you nearly everything.
References
- Bhasin S, et al. Testosterone Therapy in Men With Hypogonadism: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2018. Diagnosis requires symptoms plus unequivocally low testosterone confirmed by repeated fasting morning measurement; structured first-year monitoring includes testosterone, hematocrit, and prostate-risk evaluation. https://pubmed.ncbi.nlm.nih.gov/29562364/
- Snyder PJ, et al. Effects of Testosterone Treatment in Older Men (The Testosterone Trials). N Engl J Med. 2016. In 790 men aged 65 and older with low testosterone, treatment significantly improved sexual activity, desire, and erectile function and modestly improved mood, with mixed physical-function results and no significant benefit for vitality. https://pubmed.ncbi.nlm.nih.gov/26886521/
- Lincoff AM, et al. Cardiovascular Safety of Testosterone-Replacement Therapy (TRAVERSE). N Engl J Med. 2023. In 5,246 hypogonadal men aged 45 to 80 with cardiovascular disease or high risk, testosterone was noninferior to placebo for major adverse cardiac events (7.0 percent vs 7.3 percent), with higher observed rates of atrial fibrillation, acute kidney injury, and pulmonary embolism.
- Wiehle RD, et al. Enclomiphene citrate stimulates testosterone production while preventing oligospermia: a randomized phase II clinical trial comparing topical testosterone. Fertil Steril. 2014. Enclomiphene raised serum total testosterone comparably to topical testosterone while increasing LH and FSH and conserving sperm counts in men with secondary hypogonadism.
- FDA Issues Class-Wide Labeling Changes for Testosterone Products. U.S. Food and Drug Administration. Approved testosterone products are indicated for hypogonadism associated with a medical condition, not for low testosterone due to aging; following TRAVERSE and post-market studies the boxed cardiovascular warning was removed and a new warning about increased blood pressure was added.
- Smit DL, et al. Efficacy of human chorionic gonadotropin hormone in restoring spermatogenesis in men using non-prescribed androgens: a retrospective analysis of real-world data. F&S Reports. 2025. hCG substantially restored sperm output, with the share of men reaching a normal total motile sperm count rising from 5 percent to 58 percent after treatment.
Are TRT clinics actually legit, or is this all just a sales funnel?
Plenty of them are the real deal, staffed by licensed physicians following established prescribing guidelines. But the range is wide, from careful endocrinologists and urologists all the way down to high-volume telehealth operations that skip baseline bloodwork entirely. The filter I’d use: if a clinic will prescribe testosterone without a physical exam, lab testing, and a documented low-T diagnosis, that’s your cue to leave.
What does TRT actually cost per month, honestly?
Depends heavily on delivery method and where you get care. Injections tend to run cheaper, often somewhere in the $50 to $150 a month range just for the medication, while gels, patches, and pellets push that higher. Factor in clinic fees, monitoring labs every few months, and any add-on medications, and a realistic yearly budget lands closer to $1,500 to $3,000 for most people paying out of pocket.
What kind of TRT clinic is actually worth your time?
Depends on you, but men with straightforward low-T generally do well with a urologist or men’s health clinic that insists on thorough baseline labs, checks hematocrit and PSA regularly, and adjusts dosing based on symptoms and bloodwork together, not one or the other. Telehealth can work fine for stable, already-established patients who mainly want convenience. Physician-supervised compounding pharmacy routes, such as through FormBlends, are worth knowing about if you need customized dosing that off-the-shelf commercial products don’t cover.
How do I spot a clinic that’s just chasing high numbers instead of actually helping me?
Ask two blunt questions before you book anything: what labs do you order before prescribing, and how do you decide when my dose is actually right? A clinic worth your money is targeting symptom relief within a normal physiological range, not the biggest number it can hit. Red flags: any clinic advertising “optimal” testosterone levels well above normal reference ranges, or one that’s pushing extra add-ons at every single visit.
Written by Orla Ellison, clinical-topics writer. Reporting from the sources cited above. Last reviewed June 2026.
Shared for general knowledge. Check with a qualified provider before starting anything new.




